by Altaf Hossain, Isaac Maddow-Zimet, Meghan Ingerick, Hadayeat Ullah Bhuiyan, Michael Vlassoff, Susheela Singh
Guttmacher Institute Report, March 2017
Key points
> In 2014, an estimated 430,000 menstrual regulation procedures were performed in health facilities nationwide, representing a sharp 34% decline since 2010. The annual rate of MR was 10 per 1,000 women aged 15–49 in 2014, down from 17 in 2010.
> Some 257,000 women were treated for complications of induced abortion nationally in 2014, for a rate of six per 1,000 women aged 15–49.
> Fewer than half (42%) of public- and private-sector facilities permitted to provide MR services actually did so in 2014 (down from 57% in 2010). This proportion was particularly low among private facilities, of which only 20% reported providing MR in 2014 (down from 36% in 2010).
> Only about half of all union health and family welfare centres (UH&FWCs) provided MR procedures in 2014, a significant decline from two-thirds in 2010. These facilities are the primary health providers in rural areas, where the majority of the population lives.
> The decline in the proportion of UH&FWCs providing MR services may be due, in part, to a lack of training among younger providers recently recruited to replace a large cohort of UH&FWC providers reaching retirement age. At UH&FWCs that do not offer MR services, 92% of providers aged 20–29 reported they do not provide MR due to lack of training.
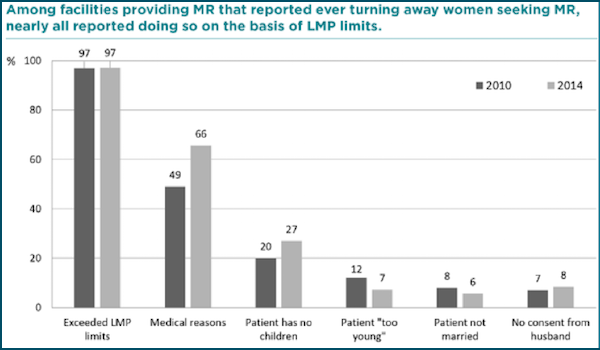
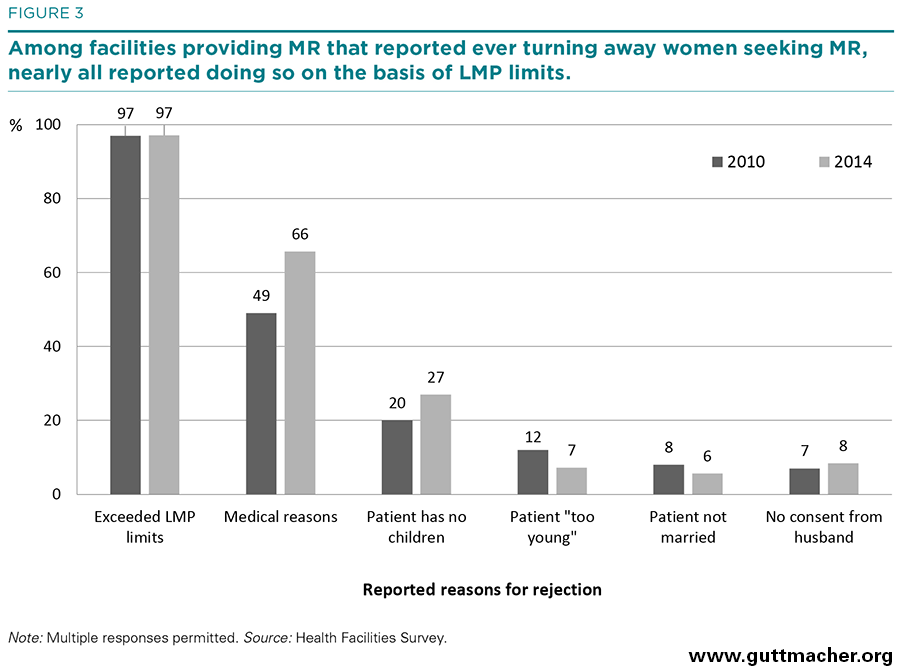
> An estimated 27% of women seeking MR services at public and private facilities were rejected. The most common reason providers gave for turning women away was having missed the window of time since last menstrual period in which MR is allowed. Many respondents also reported rejecting women for social and cultural reasons unrelated to government criteria.
> Policy and programmatic actions are needed to increase availability of and access to MR and treatment for post-abortion complications. Strategies include increasing training for providers and disseminating information about the MR program at the community level. In addition, provision of contraceptive counseling and methods for post-abortion care and MR patients must be improved, particularly at private-sector facilities.
Photo: Figure 3
{kind=link}